Blog
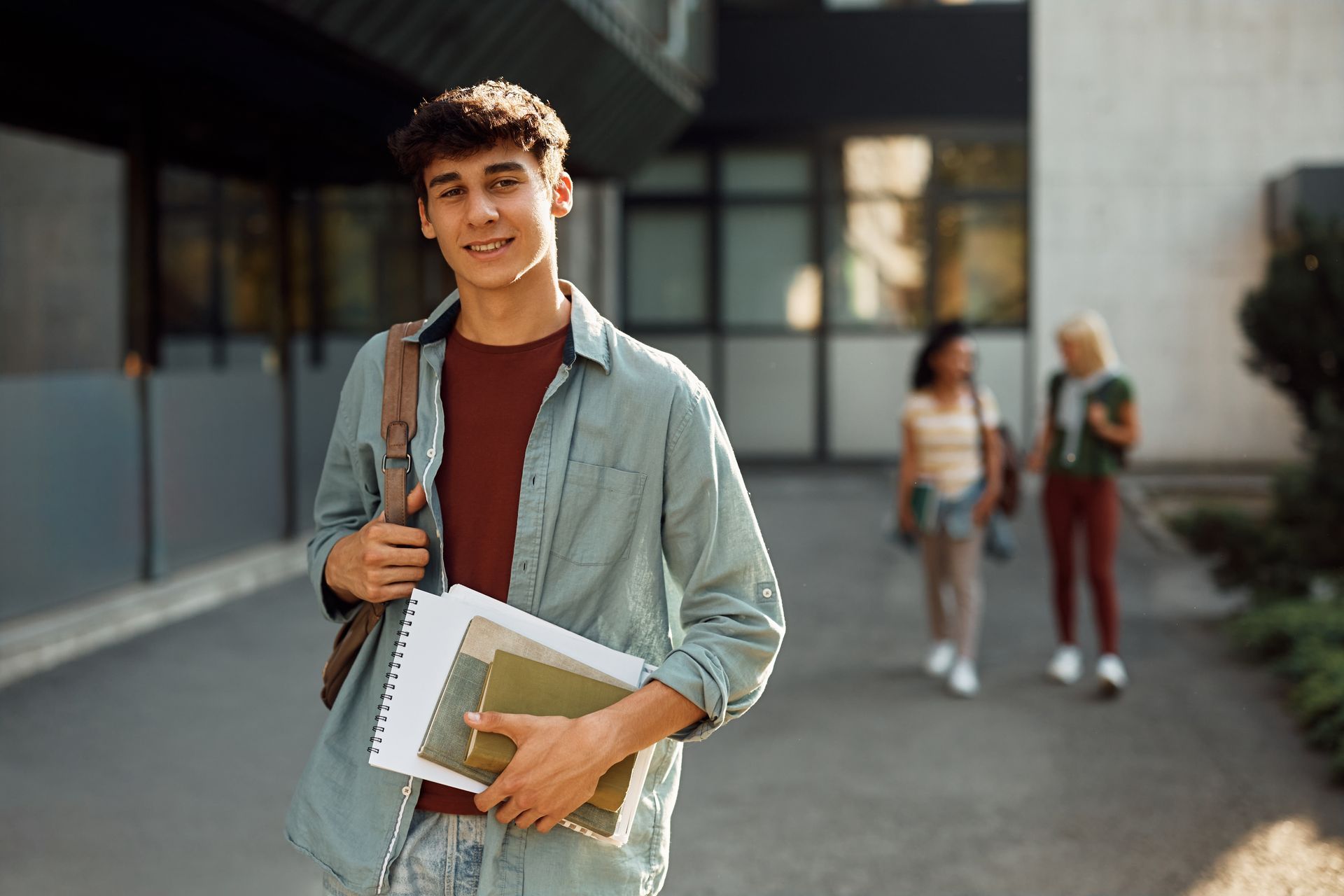
Explore the “18 cliff” and the neuropsychological challenges of transitioning to college. Learn how brain development, stress, and independence impact young adults.

Learn how diagnostic clarity helps parents understand their child’s challenges, access the right support, and create better outcomes for the whole family.
In January 2020, the American Academy of Pediatrics published updated guidelines for the identification, diagnosis and treatment of individuals on the autism spectrum . In today’s post, I walk through the behaviors that are consistent with an autism spectrum disorder. Autism Defined Autism Spectrum Disorder (ASD) is a neurodevelopmental disorder characterized by deficits in social communication/language as well as restricted repetitive behaviors (RRB). While always discussed as a “spectrum,” ASD is now the umbrella term that encompasses many previously unique or stand-alone diagnoses including: Autistic Disorder, Asperger’s Disorder, Pervasive Developmental Disorder Not Otherwise Specified (PDD-NOS), Childhood Disintegrative Disorder and Rett Disorder. While there are many opinions about the combination of these disorders, the core symptoms and diagnostic features remain largely the same. So, let’s briefly review those behaviors that are identified in each domain. Social communication deficits come in many forms. Clasically, it is described as having difficulty with the back-and-forth, or reciprocal nature of social discourse. For example, an individual may only want to talk about their own interests, or may not ask questions of the other person. Their comments may reflect thoughts in their own head, rather than be reflective or appropriate to the conversation at hand. It may be that a child has difficulty understanding sarcasm, or takes comments literally that are meant figuratively (e.g., “Don’t count your chickens before they hatch” may be challenging to understand). There are cases where an individual does not understand when to stop talking about an area of interest, while other cases where the individual is not able to initiate conversation or to join in with others. There may be difficulties with the use and understanding of gestures, nonverbal language (e.g., body language, facial expressions), and appropriateness of eye contact. Again thinking of this as a spectrum, some individuals have difficulty making and sustaining eye contact in conversations. Others may “lock eyes” onto the individual they are speaking with and may not realize when to glance briefly away. Similarly, there may be difficulties or uncertainties when engaging with peers. While some individuals with ASD may be perfectly content to play alone and do not feel compelled to seek out same-aged peers, others desperately want that form of engagement but are unsure or unskilled at securing those friendships. There are many other examples of social communication deficits, but these few examples demonstrate the vastness of the ASD spectrum. Restricted and Repetitive Behaviors are the second component of the diagnostic criteria. These may manifest as intense interest in a particular topic, repetitive actions (e.g., flicking a doll’s eyelashes, hand flapping/body rocking, lining up of toys or other objects repeatedly), insistence on sameness in the placement of objects or in the following of a daily routine, or repetitive repetition of phrases or quotes. Often these individuals have a difficult time with unexpected change, or have an intense response to a loud or sudden noise (e.g., fire alarms, car horns, large crowds). Savant skills are also captured under this domain, as often individuals on the autism spectrum are known to have incredible talents in art, math calculation (have you ever seen Dustin Hoffman in “Rainman”?) or knowledge of historical facts- among many other examples. Atypical sensory responses are also discussed under RRB . Specifically, some individuals may show reduced sensitivity to pain or may have a particularly unique response to changes in light patterns or sound. They may fixate on these interests, or may excessively touch or smell or gaze upon a particular object. Again illustrating the vastness of the spectrum, some responses are considered hypoactive (not strongly affected), while others are hyperactive (intensely responsive). Hopefully by now, the image of the “spectrum” makes more sense. Nonetheless, with the great advancements of research into identification, diagnosis and treatment, there are many wonderful, evidence-based supports for children with ASD, their siblings and families. Before delving deeper into the supports available and the typical diagnostic process, it is important to note that many individuals with ASD are deeply (and rightfully!) proud of their diagnosis. This is particularly common in those individuals previously diagnosed with Asperger’s Disorder, or those on the higher-functioning end of the spectrum. A diagnosis of ASD does not stifle or hinder them, but rather allows them to celebrate their uniqueness and gives them a space in which to feel special. While the initial diagnosis can be a shock to some families, others express a deep sense of relief that they have gained valuable insight into their family member. This knowledge is empowering, and allows families to see appropriate treatments or supports for their loved ones. Diagnosis Step one is the diagnostic process. Please check out Dr. Ghilain’s blog discussing the importance of early intervention and the tremendous outcomes that follow when individuals are properly diagnosed and subsequently provided appropriate supports early in life. To evaluate for ASD, neuropsychologists will complete a comprehensive evaluation looking at cognitive, behavioral, social and emotional functioning. It will involve interviews with parents or family members, and multiple assessments. While this may initially sound daunting, families are comforted by the amount of time we spend with them and their child, and are appreciative of the opportunity to share concerns and receive feedback. It is also not uncommon for individuals with ASD to have co-occuring diagnoses, such as Attention-Deficit/Hyperactivity Disorder (ADHD), mood difficulties (e.g., depression, anxiety) or other neurological conditions (e.g., epilepsy). Each of these components needs careful evaluation, and families need a plan for how to intervene going forward. Evidence-Based Therapeutic Interventions Once diagnosed, many evidence-based therapeutic interventions are available. “Evidence-based” is important, as this means that there is research to support not only its use with individuals on spectrum, but proof that the therapy works in the way that it claims. Unfortunately, there are many programs, classes, and interventions that tout huge impacts, with little evidence to support their claims. This can be frustrating when we hear parents share that they spent thousands of dollars on a therapy program that provided little to no benefit to their child. Our recommendations are well-established and scientifically supported. Broadly, some of the most common interventions for individuals with ASD include Applied Behavioral Analysis (ABA) therapies, or social skills groups such as the UCLA Peers Program. Just as every individual on the spectrum is unique, we tailor interventions to the child based on their personal needs. We also acknowledge that an ASD diagnosis has differential impacts on each member of the family. Siblings, parents and others may benefit from support to adjust to this new diagnostic label, interact with their child in meaningful ways, or prepare for the future. Recommendations for all family members are provided during our evaluation. So why does it seem like the rates of diagnosis are increasing so dramatically? In short, there is a better understanding of the behavioral characteristics of ASD. Therefore, parents, educators, and physicians are able to diagnose and intervene at the earliest stage possible. There is also a reduced stigma associated with the diagnosis, and many interventions available. While we have a long way to go with destigmatizing diagnoses, it appears more individuals are seeking the diagnosis for their child when the smallest concern arises. Encouragingly, there is evidence to support that some individuals “grow out of” or stop meeting diagnostic criteria for ASD as they mature. This is often associated with higher intellectual functioning, milder symptom presentations, and more intensive interventions at younger ages. While this is not the case for all children, it again is reflective of the vastness of the ASD spectrum.
The discussion of concussions has exploded in popular media in the last few years. It seems nearly every popular media site has done at least one or two pieces, sometimes many more, on the impacts of concussion and its related symptoms. In today’s blog post, Dr. Ghilain goes over the symptoms of concussion and provides readers with the facts- while dispelling common myths. What is a Concussion? A concussion is a mild blow to the head that causes a neurochemical response in the brain. It is described as neurochemical because there is no change to the physical structure of the brain itself. Common causes of concussion include falls, sports injuries (such as collisions on a football field or head-to-head contact during a soccer game), or the accidental striking of the head on an object. Typically, the initial symptoms of a concussion can include dizziness, lightheadedness, sensitivity to light or sound, nausea, feelings of fogginess, clumsiness, or other similar experiences. It is possible that the individual might lose consciousness for a brief period of time or may have difficulty recalling details about events that occurred just prior to the concussion. Neck sprains or tightened neck muscles are common and can cause stiffness and headache pain as well. All of these symptoms are completely normal, and these symptoms typically subside within a couple of weeks. If the individual is taken to an emergency department for evaluation immediately following concussion, it is unusual for a hospital to complete a brain scan (e.g., a head CT or MRI). Typically, a scan is not ordered unless the person is coming in and out of consciousness, difficult to arouse, repeatedly vomiting, or having seizures. These symptoms are indications that a more significant brain injury may have occurred. If a scan is ordered (out of an abundance of caution), brain neuroimaging is typically normal following concussion- hence why it is rarely ordered. What is important for parents/family members to realize, as well as the individual who suffered the concussion, is that the concussion sufferer will likely feel not so great for a couple of weeks. They may have difficulties sustaining focus and attention, may sleep more or less than usual, and may have ongoing headaches, light sensitivity, or general feelings of fogginess. Again, this is completely normal and will subside. It is important to know that symptoms of a concussion, while inconvenient, will go away. Individuals will recover fully from a concussion and resume a perfectly normal life. Why can recovery take longer for some people? So why is it that some individuals seem to have a concussion that goes on much longer than a few weeks? Research has demonstrated that there are five major factors that can cause an individual to experience symptoms of a concussion for longer than expected. Nonetheless, these individuals also recover fully, it just takes them a bit longer. These exacerbating factors include: a history of a learning disability attention deficit hyperactivity disorder (ADHD) a previously diagnosed concussion a history of migraine headaches a history of mood disorder (e.g., depression, anxiety) As you can see, there are many reasons why an individual may experience additional concussion symptoms for longer than a few weeks. In these cases, symptoms may last closer to a month or two, but then will subside. Myth Busting! Getting into some of the myths that are floating around popular media, while a concussion is termed a mild traumatic brain injury (mTBI), it does not mean the individual is brain damaged. It also does not mean that the individual will not recover. As discussed above, individuals recover fully from a concussion and neuroimaging (in the rarest of cases when it is ordered) is normal. A second myth is that the individual requires a dark room with little to no stimulation for weeks on end to promote recovery. In next weeks blog, Dr. Ghilain will discuss ways to support rapid recovery following concussion. Though Dr. Ghilain creates “return to sport” and “return to learn” protocols specifically tailored to the individual patients with a concussion they see, there are general things family members can do to promote recovery. While supports may be encouraged, it is important to note that these are temporary and not permanent modifications to a person’s life. Finally, during the recovery period, individuals may experience an increase in concussion symptoms while exerting themselves (e.g., when gradually returning to activities or sports or when initially returning to work or school). Though uncomfortable at times, these symptoms do not mean that the individual is further “damaging” their brain. Just like any other muscle in the body, the brain requires gradual ramping up of activities that may temporarily cause soreness (e.g., headache) or fatigue. This is not a sign that the person is re-injuring or damaging their brain in some way, it means they are on the road to recovery!
Attention Deficit Hyperactivity Disorder (ADHD) is a common disorder seen in my practice. Often co-occurring with other diagnoses such as dyslexia or epilepsy, my clients are often surprised to learn that ADHD is diagnosed based on 3 different behavioral profiles. In today’s blog, I share the 3 different types of ADHD, and the reasons why some individuals may be diagnosed as a child, while others may not be diagnosed until later adolescence or adulthood. ADHD-H: The Hyperactive Client When I think about how ADHD is portrayed in the media, the hyperactive subtype comes to mind. Perhaps you can think of someone who struggles to sit still, or acts as though they are powered by a motor! These individuals, try as they might, have difficulty containing their energy and are often moving about their space. In young children, this might be reflected in a child who bounces from toy to toy. In teenage years, this looks more subtle, such as a teen constantly tapping his or her toes or flicking a pen cap or paper clip. When able to release their energy, such as by sitting on a stability ball or shifting their weight when standing, these individuals can focus and attend to their surroundings. ADHD-I: The Inattentive Client Less well known is the Inattentive subtype of ADHD. Individuals with ADHD-I may look like they are paying attention, but they are frequently distracted. You may notice their attention is quickly pulled to other things going on in their environment, or they may look like they are zoning out or daydreaming. Often, ADHD-I is not diagnosed as early as the other subtypes, as children appear behaviorally complaint. They do not catch a teacher’s eye for being disruptive, and thus they are more likely to fly under the radar. ADHD-C: The Combined Presentation Individuals with ADHD-C struggle with both hyperactivity (ADHD-H) and inattention (ADHD-I). They are often diagnosed early because of their hyperactive traits, but upon further testing, they struggle to sustain their attention to longer or more monotonous tasks. ADHD: Behavioral Intervention or Medication? As a neuropsychologist, I am a behaviorist at heart and do not typically recommend medication as an initial treatment strategy. However, there are some clients who benefit from medication to allow them to regulate their behavior long enough to learn those behavioral strategies I recommend. While parents understandably struggle with placing their child on medication, it is often a time-limited strategy that can be removed as the child matures. Without a doubt, there are many behavioral strategies that can be implemented and tailored to a person with ADHD. To learn more about ADHD and the diagnostic process, check out my YouTube video !

When A Neuropsychologist Recommends A Section 504 Plans vs. Individualized Education Programs (IEPs)
As a neuropsychologist, I work with schools to support struggling students. I enjoy this aspect of my job, as it brings together two of my biggest academic passions: education and neuropsychology. You may not know this, but I was both a psychology and education major in college and had thought I would become a teacher after graduation. Growing up with a mom who worked as a special education teacher for over three decades, teaching just felt like it was in my blood. I worked as a substitute teacher in New Jersey when home on college breaks, and I absolutely loved working in schools. Though my career evolved from teaching to clinical neuropsychology over the years, my interest in supporting students remains to this day. So, in this blog post I want to discuss the differences between Section 504 Plans and Individualized Education Programs (IEPs). I often recommend one of these plans based on the results of my evaluation, but it is important for parents to understand the differences between these two types of service plans and why one plan may be recommended (or supported) versus another. Section 504 Plans Let’s start with a Section 504 plan. Stemming from Section 504 of the Rehabilitation Act of 1973, this federal civil rights law was put into place to stop discrimination against people with disabilities. A Section 504 Plan outlines how schools will provide support to a student who has a disability without removing the student from their classroom setting. Students who have a Section 504 plan remain with their peers, and the services are based on changes to the environment that allow students to learn or more easily access classroom material. Section 504 plans apply to any child with a disability, though the disability has to interfere with the child’s success in learning in a general education classroom setting. It is most often a written document outlining specific accommodations, supports or services for the child. Technically, it does not have to be written, but I’ve never come across a verbal Section 504 plan! There is no specific expectations around who is involved in the creation of a Section 504 plan, but often parents, a teacher, and the principal (or other school representative) are involved. Individualized Education Programs Shifting gears to an Individualized Education Program (IEP), this type of plan stems from a federal special education law for children with disabilities called the Individuals with Disabilities Education Act (or IDEA). An IEP is granted if a child has one (or more) of the 13 disabilities outlined in IDEA. You can learn more about the different classifications here. If you are looking for the full New Jersey State Regulations, check this page out for more information. The disability must negatively impact a child’s ability to learn, and the child must require specialized instruction to make progress. Often, this means the child would benefit from services outside of the general classroom setting, which may include pull-out instruction, supportive therapies (speech/language, occupational or physical therapy) or other supplemental services. The IEP is created by a very specific team of individuals, including the child’s parents, a general education and special education teacher, a school psychologist, and someone who represents the district. IEP update meetings must occur yearly, and the child is reevaluated every 3 years to be sure he or she remains eligible for services. IEP plans are formal, written documents, that include information about the child’s level of academic functioning, specific goals and progress monitoring, support services and their frequency/duration, as well as accommodations and modifications. It is important to note that an accommodation is made to a child’s environment, allowing the child to more easily access the content he or she is learning. Modifications, on the other hand, are changes to the class content or curriculum itself. With both Section 504 and IEPs, parents are notified when changes are made. While Section 504 changes do not have to be in writing, changes to an IEP must be made known to a parent in writing before they are initiated. With regard to the evaluation process that occurs every 3 years, a parent or guardian has the right to request an Independent Educational Evaluation (IEE), though the district does not have to agree to it. Similarly, a family can choose to have their child independently evaluated outside of the district, but again, the district does not have to accept the evaluation. Though I am not aware of any district “rejecting” my evaluation, I strive to be a beneficial resource to both school personnel and families. I cover all the domains that a school evaluation includes (e.g., overall intellectual functioning, academics, social and emotional functioning), but extend the evaluation to include measures of executive functions, memory, language and visuospatial functioning, adaptive functions or daily independence, etc. You can read more about the IEE process by clicking here . Overall, Section 504 Plans and IEPs provide different types of services and supports to children who need them. It is best when parents and school personnel can agree to these plans without conflict, but there are formal processes that can be initiated if disputes arise. Hopefully, if you are reading this blog, those processes do not pertain to you! As this new school year begins, I wish all families, educators, and students a happy and successful year ahead!

When an individual comes for a neuropsychological evaluation, they are often unsure of what exactly to expect. In today’s blog post, I will review what to expect during a neuropsychological evaluation: from scheduling through feedback! Initial Phone Consultation & Appointment Scheduling: Typically, a family member will call to request an appointment, either for themselves or for a loved one. At this time, I will ask about current concerns, explain the steps of the evaluation, and schedule the appointment. This is a great time for family members to ask questions and learn more about the process. Intake Appointment: I schedule the 1-hour intake interview with the client (or parent) approximately 1-2 days before the full-day evaluation. During this HIPAA-secure video call, I will ask about current concerns, gather the client’s history (e.g., medical history, educational history, etc.) and further outline what to expect on the evaluation day. For those that prefer, the intake interview can occur on the day of the evaluation, but I find that most families welcome the opportunity to speak candidly about their concerns from the comfort of their own homes. Evaluation Day: Evaluations last from approximately 9:00 in the morning to mid/late afternoon. I block the full day for the client, leaving ample time for rest breaks, brain breaks, and lunch! The client spends the day completing various tests or activities, including paper and pencil tasks, iPad tasks or computerized tasks that assess the different ways the brain is working. I assess memory, speed of processing, language, attention- the list goes on! The evaluations are comprehensive in order to gain a full picture of the individual’s thinking, learning, emotions and behavior. Report & Feedback: Within 2 weeks, a comprehensive report is provided to the client or family. This includes information gathered during the initial interview, the results of the testing, a summary and integration of findings, provision of any diagnoses I feel are appropriate, as well as a list of home, school/vocational, and community-based recommendations. I most often schedule a video conference to review the report and my recommendations, though clients are welcome to return to the office if they would prefer to review the results in person. I want to be sure the information makes sense, and that families feel well-equipped to navigate the recommendations provided. Though the evaluation is typically a one-day process, I remain available to clients, families and their related service providers to answer questions, discuss recommendations, consult with schools, and provide support. I am happy to hear when clients or family members are thriving, and equally as motivated to assist if future challenges arise. I am grateful to families for entrusting me with the care of their loved one. I look forward to an ongoing partnership – here’s to many successes ahead!

Welcome to Brain Health Neuropsychology! My name is Dr. Christine Ghilain and I am a board-certified clinical neuropsychologist in private practice. I wanted toy introduce myself, and to walk through some of the key pages on my website where you can find information about the clients I serve and the services I provide. A Review of the Website To begin, the home page welcomes you to the site, and points out those unique qualifications that separate me from other neuropsychologists who might have popped up on your google search. To that end, clicking on Meet Dr. Ghilain gives you more information about my education and q ualifications as a neuropsychologist, some of the most common neurological or developmental conditions I see in my practice, as well as a selection of recent talks and presentations I gave at national and international conferences. I include this information so that you can feel confident that I attained the appropriate training and have the skills necessary to serve you or your family’s needs. I’ll touch on conscious consumerism in a future blog! Unfortunately, there are some individuals who call themselves neuropsychologists who have not met even the minimum standards of competence in the field. Thus, I am happy to be transparent about my background and training. So what is neuropsychology all about? Some of the first questions I answer when clients call to schedule with me include: (1) what exactly is a neuropsychological evaluation , and (2) why would someone need to seek out a neuropsychologist for an evaluation? Therefore, I included pages on the site discussing those two very common questions! I include other common questions that arise when individuals call to learn more about the process, and I am always glad to talk through additional concerns of family members. Future blog posts will address these two main questions, but for now, clicking the links to learn answers to those questions. I see individuals for evaluations across two broad categories: clinical and forensic. Clinical evaluations are for individuals who notice changes to their thinking, learning or productivity, or for those who struggle at school or work. For infants, this may be due to an early stroke in utero or delayed developmental milestones. For preschool-aged children, this evaluation can provide an understanding of whether the child is ready for kindergarten, or if they need to be set up with a school support as they enter elementary school. Across late childhood and teenage years, I see clients whose parents are concerned for attention difficulties, disorganization, sadness, worrying, or learning challenges (amongst many other things!). In adulthood, I see individuals who may have struggled their whole life with difficulties socializing or maintaining consistent employment. Others may have suffered a stroke or brain injury, and want to understand how their injury may impact their functioning as they age. Finally, in older adulthood, clients see me with concerns for dementia, changes to their mood, or difficulties at work. A family member can also bring them due to personality changes, for example. Often, an individual who is diagnosed with a neurological or developmental condition comes to me to understand how they can maximize their success in the context of their diagnosis. My goal is to empower clients to use their areas of strength to bolster areas of weakness. My clients leave with a roadmap for exactly how to do just that! On the forensic side, I see clients who have known or suspected brain injury or insult as a result of an accident or incident. They may be seeking financial compensation, or they may be referred by their insurance company in order to determine their eligibility for disability benefits. Finally, I am often retained by school districts to complete Independent Educational Evaluations. These evaluations support schools in providing the best services for their students. In the final pages of this site, I answer frequently asked questions, blog about new topics of interest, and provide a method for interested individuals to contact me for consultation . I look forward to providing more information in the weeks, months and years ahead!